Hemodynamic Instability
What is hemodynamic instability?
The study of blood circulation is clinically termed as ‘ hemodynamics’. The compromise blood circulated is cause of hemodynamic instability, which is usually associated with hypotension (lower blood pressure than the normal). Untreated condition causes tissue necrosis or cell death and consequently multiple organ failure.
Abnormal hemodynamic parameters including, blood pressure, heart rate, cardiac output, pulmonary artery pressure, central venous pressure and pulmonary artery occlusion pressure can be control by providing proper medical intervention and close monitoring , which help to stabilize hemodynamic parameter/s and restore the organ perfusion.
Blood pressure and mixed venous hemoglobin oxygen saturation (SvO2) or cardiac output are two variables, which has direct influence on organ perfusion.
Hypotension can produce insufficient perfusion in the brain and heart due to autoregulation of these organs. The individual is mostly affected, when the particular threshold of the blood pressure become drop down and may cause cerebral and coronary ischemia. (1,2)
Symptoms
The symptoms of the hemodynamic parameters are similar as shock, which include:
- Hypotension
- Abnormal heart rate
- Cold extremities
- Peripheral cyanosis
- Decreased urine flow
- Alternative consciousness
- Chest pain (1)
Who is at risk?
Hemodynamic instability is common during surgery conducted under general anesthesia. An anesthesiologist is continuously monitoring the patient for maintaining the normal hemodynamic. Usually anesthesiologist plan a clinical management before commencing the surgery, depending upon the pre-existing condition of the patient.
For made an effective plan for hemodynamic management, it is necessary to have thorough knowledge of medical history. The risk of hemodynamic instability is more with patient having cardiovascular diseases and major surgery need relatively more complex planning for hemodynamic management than healthy patient. (2)
Recognizing hemodynamic instability
For recognizing the critically ill patient and avoidance of hemodynamic instability, the following diagnostic tests should pursue:
Clinical assessment in the seriously ailing is mainly utilized for the initial three rationales: for example to decide whether the individual patient has hemodynamic instability, to decide whether the individual patient is countering to treatment and to stratify threat of instability.
When a healthcare staff checking the systolic BP (blood pressure) or vessels fills up time the measuring of the result should be exact, precise, and offer further direction to specify the presence of any cardiac syndrome. If the obtained result provides any information which can direct the clinician about the presence of hemodynamic instability or shock, then it is easier to make some decision about the management of the hemodynamic instability, before onset of the condition.(2)
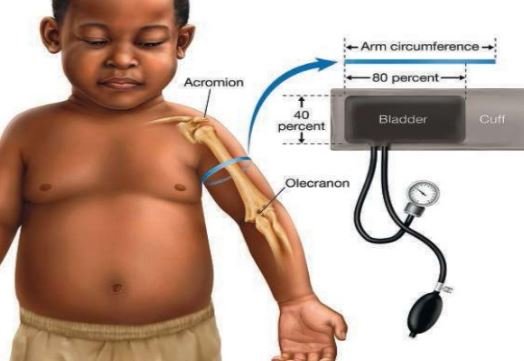
Fig 1 – Blood pressure recording
Method of clinical assessment of Hemodynamic Instability
The assessment of vital sign and surrogate bio markers for assessing the organ perfusion, including urine output and capillary refill time have frequently used clinical assessment method to estimate hemodynamic instability. The below mentioned techniques are used as diagnostic tests for hemodynamic instability.
Vital signs
The monitoring of the vital signs is the primary clinical assessment for evaluating hemodynamic instability of a patient. Vital signs measurement is very important in judging the severity of the patient’s condition and to decide the any emergency medical intervention need to support for life saving of the patient or not. The following are the included elements of the vital signs.
Pulse
Variation of pulse rate may provide initial symptom of the development of the hemodynamic instability. The factors which mainly affect the pulse rate are fever, physical exhaustion or exercise, disorder of the thyroid gland and certain medications.
The increase level of catecholamine hormone during stress, haemorrage or dehydrations are different causes which influence pulse rate. The postural alteration can affect pulse rate and provide the indication of hypovolemia. Increase or decrease rate of pulse is a marker for arranging of a medical emergency team.
Respiratory rate
Respiratory rate is an important element to assessing the hemodynamic instability, as it is a marker of severity of illness. Respiratory rate become drop down for acute respiratory failure and immediate emergency medical assistance is required to manage the patient ill health. Respiratory rate also provides guidance of patient reaction after giving any therapy.
Mean Arterial Pressure / Blood Pressure
Proper maintenance of the blood pressure is required to maintain the autoregulation of the heart and brain by keeping sustain perfusion. Mean Arterial Pressure / Blood Pressure is a good marker of hemodynamic instability. Less than 90 mm Hg in systolic blood pressure or less than 65 mm Hg of Mean Arterial Pressure indicates severe sepsis and septic shock.
Temperature
High body temperature is also used as an indicator of clinical condition of the patient, though it is not sensitive marker of hemodynamic instability.
Toe- Temperature Gradient
Most of the clinicians suggest Toe- Temperature or rectal temperature gradient is useful diagnostic measure for adequacy of circulation. Toe- Temperature Gradient is a better indicator than Mean Arterial Pressure, cardiac index or lactate to discriminate between survivors or non survivors for patient admitted to a ICU.
Organ perfusion
Organ perfusion is very important marker for diagnosing hemodynamic instability. hypoperfusion in specific organ indicative of insufficient perfusion in kidney or cardiac output.
Urine Output
The small quantity of urine production (oliguria) is another way to diagnose hemodynamic instability, but may associate with other clinical conditions, so it is an important but not specific clinical marker for hemodynamic instability. insufficient renal perfusion is one of the cause of oliguria. 0.5ml/kg/hour urine output is a sarogate marker for severe sepsis.
Capillary refill time (CRT)
This clinical element is used to diagnosis the severity of instability of a patient treating under emergency care unit or ICU. The CRT is usually measure by preseeing the finger nail bed to occlute the circulation and then release the pressure and time is noted for how long normal coloration is achieved. CRT more than 6 seconds indicates emergency condition. The abnormal level of CRT along with cardiac index and urine output may indicate acute lung injury. (3,4)
References
- M.H Weil (2005); Defining Hemodynamic Instability; Retrieve from: http://link.springer.com/chapter/10.1007/3-540-26900-2_2#page-1
- James Bailey (2003); Hemodynamic instability; Retrieve from: file:///C:/Users/Abjijeet/Downloads/Hemodynamic%20instability_DOC0988423_070411.pdf
- Sevransky J. Clinical assessment of hemodynamically unstable patients. Curr Opin Crit Care. 2009 Jun;15(3):234-8. Retrieve from: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2849135/
- http://www.virtualmedstudent.com/links/cardiovascular/hemodynamically_unstable_patient.html